
Sepsis is life threatening…if concerned, seek advice immediately and ask #coulditbesepsis?
Get help
A big congratulations to A/Prof Naomi Hammond, Head, Critical Care Program and Sepsis Australia at The George institute for Global Health, for her appointment to Executive Director of Research, Northen Sydney Local Health District (NSLHD). In addition to this recent appointment, Naomi received the Chief Executive Commendation Award at the NSLHD 2023 Exceptional People Awards ceremony.
Naomi’s expertise and wealth of knowledge continually solidifies her position as a leading health researcher in Australia. We are so grateful and lucky to have you Naomi – thank you for your ongoing dedication and commitment in pursuit of excellence in healthcare.
Sepsis Australia would like to would like to express our sincerest gratitude to GAMA Healthcare Australia for their generous donations and continuous charity work to support the unfunded program of Sepsis Australia. We deeply appreciate GAMA’s commitment to our cause and the impact it will have on the fight against sepsis. In the last 12 months, GAMA Australia have contributed significant funding to Sepsis Australia. Every contribution helps our mission to improve sepsis recognition and clinical care, establish support to foster better outcomes for survivors, and reduce the burden of sepsis in Australia.
Check out the incredible charity work of GAMA below and how they continually think of creative and innovative ways to raise funds for such an important cause.
Thank you GAMA Healthcare, we are so grateful for your ongoing support!
Over the past 12 months, GAMA hosted one event per quarter and along with a Trivia and other challenges.

GAMA’s phenomenal team in Australia dusted off their camera’s and snapped some amazing photographic masterpieces. There were 3 winners who each won a $100 gift voucher and some of the photos which resulted were simply stunning.
GAMA encouraged their employees to clear out their wardrobes and bring any old clothing, blankets, bedding, etc into the office. These donations were then packed up and delivered to the Salvation Army in Melbourne to distribute to those who may need some extra support this winter.

GAMA celebrated World Sepsis Day on 13th September 2023, by holding a “Pink Picnic”. The team celebrated by having a picnic lunch outside in the sunshine.
To find out more information about GAMA Healthcare, click here.
The George Institute/Sepsis Australia and the Australian Commission on Safety and Quality in Health Care are currently planning for the National Sepsis Program (Phase 2 ‘Extension’) that will build on the work achieved in the National Sepsis Program (Phase 1) which saw the launch of the national Sepsis Clinical care Standard. March 2024 is the planned commencement for the Phase 2 program will comprise of five key projects:
Program Governance will include the:
Regular updates will be provided each month to keep you up to date.
In the meantime for more information see:
https://www.safetyandquality.gov.au/our-work/national-sepsis-program
In honour of International Day of Women and Girls in Science on Sunday 11th February, we’re celebrating the success of Dr Amy Freeman-Sanderson and Sepsis Australia, Program Head Associate Professor Naomi Hammond.
Dr Amy Freeman-Sanderson (from University of Technology Sydney) was recently awarded the 2024 Australian Critical Care Excellence in Research Award, from Australian College of Critical Care Nurses, for the article ‘Communication functions of adult patients admitted to intensive care: A multicentre, binational point prevalence study.’ People who experience sepsis are often admitted to the ICU and Amy’s study looked at the profound impact on communication for patients during their stay in the ICU. Read more about Amy’s article here.
In November last year, A/Prof Naomi Hammond was named in The Australian’s 2024 Research magazine as the nation’s leading researcher in the field of critical care. Naomi’s research collaborations into the use of intravenous fluids for critically ill patients has transformed how medical staff use fluids for resuscitation and the types of fluids that are used. Read more about Naomi’s work here.
We’re so very grateful to have remarkable women like Amy and Naomi working to improve the outcomes for people who are admitted to the ICU.
After a small scratch from his puppy, Jake developed a drug-resistant infection, which lead to sepsis. Read more about Jake’s experience, the rise of antimicrobial resistance and the overuse of antibiotics in Australia, here.
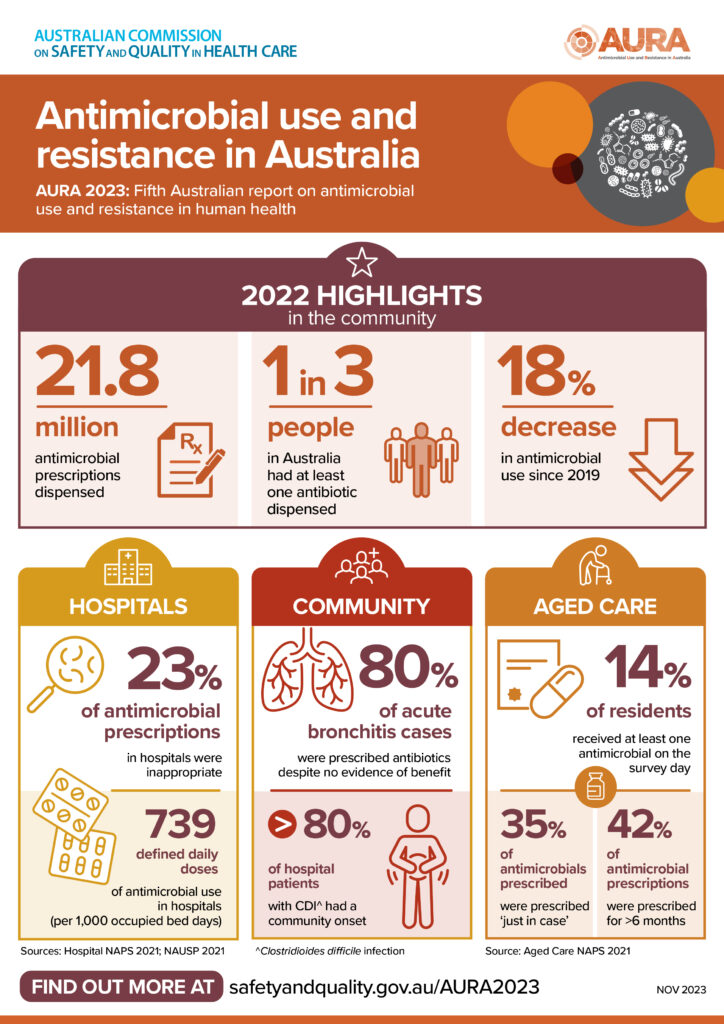
The nation’s latest major report on antimicrobial use and resistances has revealed that Australia is heading in the right direction – but there’s still a lot of work to do.
AURA 2023: Fifth Australian report on antimicrobial use and resistance in human health was released by the Australian Commission on Safety and Quality in Health Care on 16 November 2023.
The report highlights trends and analyses in antimicrobial use in hospitals, aged care and primary care settings, as well as changes in resistance that are important for infection prevention and control, and antimicrobial prescribing.
Early treatment with antibiotics can stop sepsis & antimicrobial resistance can be avoided with good antimicrobial stewardship.
Find out more and read the full report here.
Last week a report from the from the UK National Health Service (NHS) ombudsman warned that sepsis is still killing too many patients. The report details avoidable mistakes and makes recommendations to improve patient safety. Read the full article from the Guardian.
Sepsis Australia Program Head, Associate Professor Naomi Hammond commented:
“The parliamentary and health service ombudsman (PHSO) report of sepsis cases in the NHS is an all too familiar story across healthcare settings globally. In an effort to improve recognition and response to sepsis in the Australian healthcare system, a National Sepsis Clinical Care Standard has been developed and released by the Australian Commission on Safety and Quality in Healthcare in partnership with Sepsis Australia and The George Institute for Global Health. The goal of the sepsis standard is to ensure patients presenting to any health care setting with signs and symptoms of sepsis receive the optimal care, from symptom onset through to discharge from hospital into the community.”
Find out more about the National Sepsis Clinical Care Standard.
Sepsis Australia Advocacy Group member, Mandy, discusses her experience of Strep A and sepsis in this clip from The Project. We also hear from infectious disease expert Professor Sanjaya Senanayake about the symptoms and signs to look out for.
Mandy and fellow amputee, Korrin Barrett now run the Quad Squad – the world’s only support group for people specifically missing all four limbs. The Quad Squad meets biannually in Australia and is a place where quadruple amputees share tips, ideas, hear from industry experts and support one another.
You can get in touch with Mandy or the Quad Squad through her website or Facebook.
Sepsis Survivor, Caitlin Alsop, nearly lost her life to a dental infection. Five years on she has launched the FACE Sepsis Project. A pioneering dental sepsis education program for dental and primary care, developed by Caitlin in partnership with Sepsis Australia.
Click here to find out more and book Caitlin for your staff training.
This research project is a phenomenological study seeking to understand the lived experience and perception of non-clinical persons who are ‘known and familiar’ with an older adult who has been diagnosed with sepsis. Interviewing with each individual participant is expected to take an average 45-60 mins. The benefit and potential impact in doing this specific research is the following:
All of this being consistent with this contemporary movement on patient and consumer involvement.
For more information please see the Participant Information Sheet at: Participant Interview_Information_Sheet
