
Sepsis is life threatening…if concerned, seek advice immediately and ask #coulditbesepsis?
Get help
This week: Professor Tex Kissoon, President Global Sepsis Alliance presents ‘Decreasing Burden Through Prevention’
The Pocketbook of Sepsis is launching in January 2023: Global experts, Global Impact.
The burden imposed by sepsis in Switzerland contrasts with the lack in public awareness, insufficient
institutional efforts to reduce sepsis, as well as absence of national coordination and monitoring to
reduce the impact of sepsis. Sepsis has often been called a disease of systematic failure to
learn.
Root-cause-analyses of patients who die of sepsis commonly reveal reoccurring patterns of
delayed presentation by patients and families due to lack of awareness, delayed recognition by
healthcare staff, and missed opportunities for effective interventions once sepsis is recognized. In
addition, survivors and family members are often left poorly informed about sepsis and its long-term
sequelae which are not appropriately addressed by existing support structures. Other healthcare
systems have summarized these challenges unique to sepsis as the combined effect of a lack of:
– Awareness and education of the public and healthcare workforce
– Standards and pathways for sepsis recognition and treatment
– Follow-up systems for survivor and family support and rehabilitation
In response to that gap, recently, a group of sepsis experts across Switzerland formed a national
multidisciplinary panel to identify the need, gaps, and strategies to address sepsis in Switzerland.
Subsequently, in June 2022 key stakeholders convened at a policy roundtable in Berne
to address the pressing need to improve awareness, prevention, and treatment of sepsis in
Switzerland. Participants included clinical, academic and policy professionals as well as sepsis
survivors from different regions in Switzerland.
The format and processes used to convene the round table and reach consensus on national priorities, to inform the SWISS Sepsis National Action Plan 2022, were based on those used by Sepsis Australia (then the Australian Sepsis Network) in 2017 to Australian Stopping Sepsis National Action Plan https://www.australiansepsisnetwork.net.au/home/ssnap-2
The goal of the roundtable was to formulate a set of consensus recommendations towards creating a Sepsis National Action Plan in Switzerland. The report Swiss Sepsis National Action Plan (SSNAP) September 2022 sets out an action plan to drive improvements in the treatment and recovery of patients with sepsis focusing on four overarching recommendations:
1. Launch a sepsis awareness and education campaign targeting the public, as well as the healthcare workforce.
2. Establish and implement a minimal national standard for the detection, treatment, and follow-up of sepsis.
3. Establish and implement support systems for sepsis survivors and for families affected by sepsis.
4. Promote national sepsis research including healthcare service, translational, and basic science research.
These overarching priorities reflect not only the Australian experience but also global priorities stipulated in the 2017 World Health Assembly Sepsis Resolution 70.7.
Read more here: Swiss-Sepsis-Action-Plan 2022
Sepsis kills 11 million people every year, often due to the lack of safe & effective antimicrobials to treat it.
The best defence against sepsis is strong health systems.
On World Sepsis Day, WHO calls on countries to deliver safer, cleaner & better quality care to save lives.
See more at: WHO WSD Video
World Sepsis Day is 13 SEPT 2022
Thankyou to our local sepsis champions and consumer advocates who work tirelessly to improve outcomes for #sepsis survivors, their families and carers.
Join us on World Sepsis Day to raise awareness https://www.worldsepsisday.org/wsd2022



The Australian Commission on Safety and Quality in Health Care, in partnership with The George Institute Australian Sepsis Network have developed a national Sepsis Clinical Care Standard to improve the delivery of sepsis care in Australia. The goal of the Sepsis Clinical Care Standard is to ensure a patient presenting with signs and symptoms of sepsis receives prompt optimal clinical care, from symptom onset through to discharge from hospital into community care. This includes timely recognition of sepsis, early and appropriate antimicrobial therapy and continuity of care from the acute setting through to their discharge and recovery. Establishing a nationally recognised clinical standard of care for sepsis was a key recommendation in the Stopping Sepsis: A national action plan report and one of eight projects commissioned under the National Sepsis Program.
For more details see: https://www.georgeinstitute.org/media-releases/new-standard-is-a-game-changer-that-will-ensure-healthcare-workers-recognise-sepsis
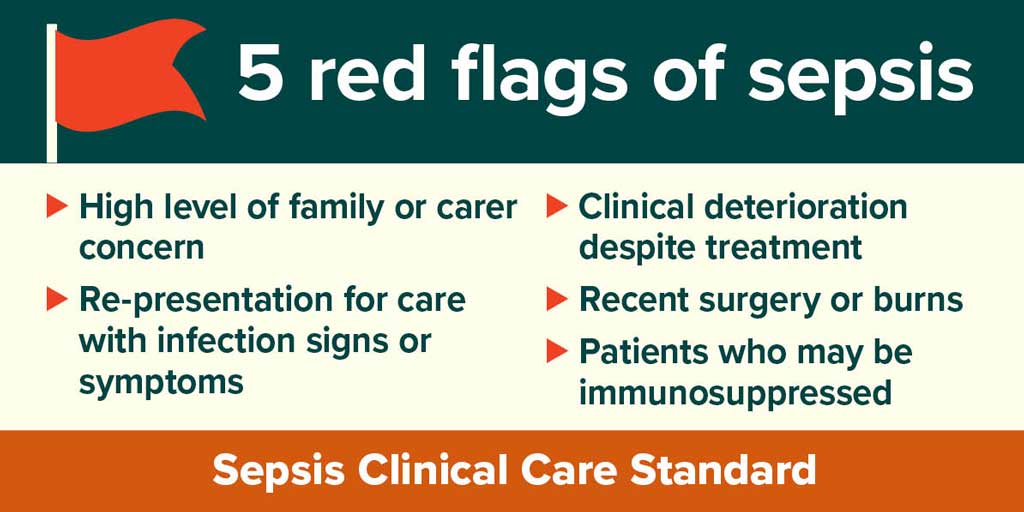


The Australian Commission on Safety and Quality in Health Care in partnership with The George Institute for Global Health Australian Sepsis Network has developed a Sepsis Clinical Care Standard to provide guidance to clinicians and health service organisations when investigating and managing sepsis, and information to consumers about the care they can expect to receive.
The launch of the SCCS was hosted by Ms Julie McCrossin AM, Broadcaster and Commentator, the panellists include:
The SCCS was formally by Professor Villis Marshall AC, Chair of the Board of the Australian Commission on Safety and Quality in Health Care.
Watch the launch at: https://youtu.be/gt_JnxR2TXk
UQ leads global trial of new sepsis treatment – an international clinical study, led by University of Queensland, is examining new ways of treating children with sepsis using vitamin C and steroids alongside antibiotics.
Listen to the podcast featuring: Mia Wilkinson, sepsis survivor, Ellie Wilkinson, Amy Wilkinson
Dr Sainath Raman, senior research fellow, Child Health Research Centre
RN Breakfast with Patricia Karvelas
The Queensland Paediatric Sepsis Program is excited to release the ‘The Sepsis Connection’.
The Sepsis Connection is a newsletter that is ‘for you and from you’. Developed by our team of Advanced Social Workers, it aims to create connections within the paediatric sepsis community by sharing stories, information and resources that may be of use to families.
The quarterly newsletter will be distributed electronically to those who are registered with the QPSP Family Support Network. The Family Support Network is available state-wide, and all families of children that have been affected by sepsis are invited to join.
If your family may benefit from the Sepsis Connection, please register with the QPSP HERE
The Queensland Paediatric Sepsis Program Peer Mentor Program aims to provide families with the unique understanding, encouragement and support which only another parent who has walked a similar path can provide. The program can be offered to any family within Queensland as the support is provided via phone and email.
Peer Mentors are parents and carers who have been referred by a staff member, family at Children’s Health Queensland or self-referred as someone who would like to provide peer support and information on “navigating the journey” of sepsis treatment and medical care or bereavement. Peer Mentors are required to participate in extensive training prior to commencement and continue to be provided with ongoing support and supervision by Peer Mentor Program Leads throughout their time with the program.
Peer Mentors have first-hand experience with:
If you would like to register to be a Peer Mentor and provide support to other parents and carers, or you are a parent or carer with a child newly diagnosed with sepsis and would like to be linked with a Peer Mentor please click HERE
In strong partnership with consumers, the Queensland Paediatric Sepsis Project (QPSP) aims to deliver a world leading holistic approach to paediatric sepsis within the acute care setting and beyond, including development of a comprehensive education and awareness platform; expansion of the sepsis pathway into inpatient areas of care; an integrated model of care for post-sepsis support; a family support network and peer mentor program for families of children diagnosed with sepsis; initiatives to support communication and care inclusive of culturally and linguistically diverse families; and champion health equity for Queensland’s Aboriginal and Torres Strait Islander infants, children, young people, families and communities.
Sustainability is a key focus for all activities of the program. The QPSP created a 5-year roadmap to tackle sustainability issues, particularly in relation to embedding pathways into clinical practice, improving sepsis management, family experience and outcomes, and improving health service efficiency and effectiveness.
For more information see: QPSP Sustainability Report Communique APR 2022